Dentistry has advanced so much recently, especially in dental bonding. Previously, it was more common to use amalgam restorations to replace decayed (cavitated) tooth structure. However, these restorations were not desirable in color and purely relied on mechanical retention. As a result, they were not aesthetic and there was a risk of fracture in the long-term. This doesn’t mean that it doesn’t have its place in dentistry. As a matter of fact, amalgam restorations are desirable when restoring teeth that lack the ability to isolate properly.
Currently, the majority of teeth restored from decay are composite restorations. These are resin based restorations that not only have mechanical retention, but also a chemical bond. This allows for a stronger bond to the tooth that mimics natural tooth structure. However, using dental composites are very technique sensitive and must be done in proper isolation to allow for the full bonding benefits. Another obvious benefit of resin composites is the aesthetics. We can customize the shades of composites, and so we can very closely mimic the shade of tooth to allow for high aesthetic results.
Because of these advances in composites, it has allowed us to use utilize treatment that better satisfies the needs of more difficult cases.
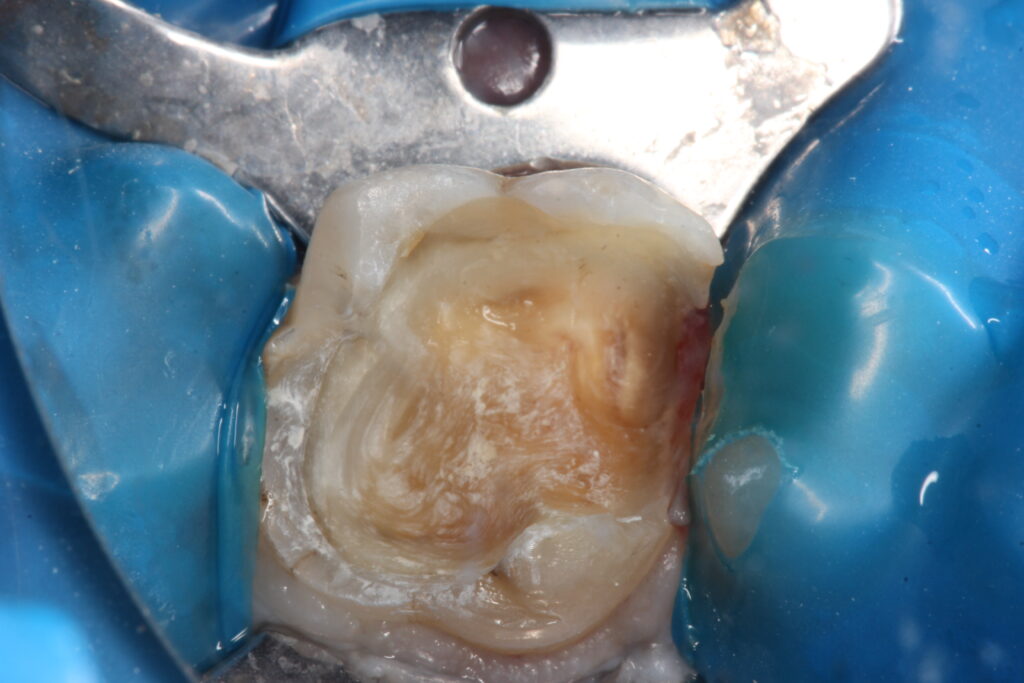
In this case, we are presented with a large amalgam (silver) restoration. This restoration held well for many years. However, there appears to be some leakage in the restoration and you can see that with the gaps between the tooth structure and “filling” material. In these gaps, bacteria will seep in and build up to cause caries. Because of this we decided to remove the old restoration, and remove the existing caries. Because of all of the existing caries, we were left in a dilemma. Will this tooth be able to withstand occlusal load (biting, etc.) if restored with a composite restoration? Or will it require a crown?
We decided to restore this tooth with a composite restoration for a couple of reasons. First, the decay had extended close to mesial pulp (the “nerve”). If we protect the tooth with a crown and soon after the patient becomes symptoamtic, we will have done a crown prematurely before root canal treatment would have been recommended. As a result, future root canal therapy would possibly done through the new crown. Second, restoring it with composite would allow us to buy some time and determine if the tooth does become symptomatic. Our last factor in deciding to utilize composite material was the size of the tooth. The patient’s tooth was small. During the process of a crown prep, we would need to remove much tooth structure to allow enough room for the crown material. We decided that being conservative in this case would be best for this case.
There are many factors involved in deciding treatment. It isn’t so simple as “drill, fill, and ….”.
Smile on